
Inflammation of the iliopsoas muscle
What is the Illiopsoas muscle?
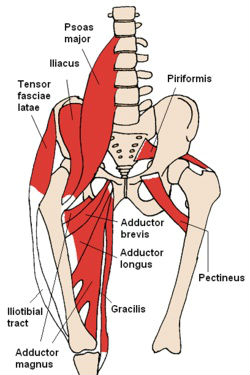
The iliopsoas muscle is a very strong muscle that lifts the knee up and controls/supports postural changes. The iliopsoas is important for standing, walking, and running.
The term iliopsoas refers to the combination of the psoas major and the iliacus at their inferior ends. It starts at the lower back and inserts into the thigh bone (femur). This muscle can become inflammed if overworked with situps especially with a weight behind ones' neck, or excessive uphill running. Behind the muscle is a bursa that can become inflammed on it's own or along with the tendon.
 Illiopsoas muscle
Illiopsoas muscle
Symptoms include:
Pain in the groin when you lift your knee up to your chest particularly against resistance. A sensation of tightness and swelling in the groin - especially if the bursa is involved. You might enter a cycle of pain where the pain disappears during training only to recur worse after exercise has stopped.
What can the athlete do?
Rest until there is no pain. Apply heat in the form of a hot water bottle and use a heat retainer. Stretch the hip flexor muscles. See a sports injury professional who can advise on rehabilitation and strengthening.
What can a sports injury specialist or doctor do?
Prescribe anti-inflammatory medication e.g. ibuprofen. Use ultrasound. Prescribe a rehabilitation and stretching programme. Give a steroid injection.
If you have pain in the groin you must rest immediately or it could develop into a chronic condition that is very difficult to treat.
Source: Sports Injury Clinic
========================================================================================================
The Iliopsoas Muscle -- The Great Pretender
The description is appropriate. The iliopsoas muscle is a major body mover but seldom considered as a source of pain. It mimics low back pain, hip pain, and leg pain individually or in combination.
Have you ever had a patient with classic lumbar sprain/strain symptoms that didn't seem to get better in a reasonably short time? No matter what adjustments or therapy you administered, did the condition gradually worsen? Did it seem to spread to surrounding areas in the hips, legs, and thoracic regions? The chances are you were dealing with an iliopsoas muscle spasm. It often accompanies other conditions affecting the low back.
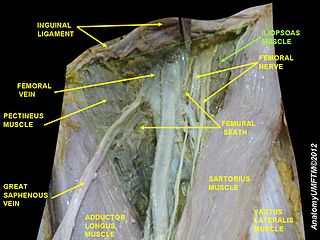
It's very important to understand the anatomy involved. The iliopsoas muscle is comprised of two parts. The iliacus and psoas muscles are joined to each other laterally along the psoas tendon. The iliopsoas originates anterior to the transverse processes of the T12 to L5 vertebrae and inserts into the lesser trochanter of the femur. Both are innervated by the 1st through 3rd lumbar nerve roots. As a combined muscle it is a major flexor of the trunk at the pelvis. In fact, it is considered the most powerful flexor of the thigh. It traverses the body internally, and is only accessible in a very small area in what is known as the femoral triangle, where it inserts into the lesser trochanter of the femur.
This location, major action and inaccessibility account for it being a great pretender. Since it originates anterior to the transverse processes and angles internally there is no therapy which will penetrate deep enough to affect it from the posterior. The lumbar attachment and innervation account for the pain felt in the posterior lumbar region. Because it is a major flexor, if it is in spasm, it will cause many of the regional muscles to compensate and become overused, hypertonic, spasmodic and painful in their own right. Since it is a muscle not known nor understood by most people, it is difficult for most patient to describe the location any more specifically than the low back.
Classic symptoms of an iliopsoas muscle spasm are diffuse achy- type low back pain of a few days onset. The history is generally not specific to an injury which would be considered for low back pain, but it can be. The pain seems to spread to the rest of the low back, lower thoracic and even into the gluteal and lateral hip regions. Most often a key factor is initial pain upon rising from a seated position which may dissipate in a short time. It is difficult to stand upright quickly. Standing, walking and laying down don't seem to affect it badly. Occasionally there may be pelvic discomfort and bowel complications in the history. Relief of pain is often experienced by sitting down. However, extending the leg, as in driving, can make the pain worse. The types of physical actions which seem to cause this condition are standing and twisting at the waist without moving the feet; any action which causes the leg to externally rotate while in normal extension; and even doing too many sit ups (this is the muscle which completes the last half of a sit up).
A few simple tests are in order. Since the action and position are specific, have the person externally rotate their leg and foot 90° and extend it backward with the knee straight and the forward knee flexed and pelvis straight. (Think of kicking a soccer ball with the instep of the foot while doing a fencing forward thrust). This may produce minor pain. Have the person lie on their back and raise and hold both legs 12 inches off the table. This may produce pain, but usually a weakness, especially on the injured side. Have the patient do a sit up against resistance at the 45° position. This should produce some moderate pain in the groin area. The most positive diagnostic test is to have the person flex the knee, hip and externally rotate the leg, such that the lateral malleolus is laying on top of the contralateral knee. Palpate the femoral triangle deeply (press with a single finger 3/4 to 1 inch deep) and look for a reaction. Do this over an area enclosed within the femoral triangle, not just in one spot. If the iliopsoas muscle is in spasm the patient will jump off the table. Believe me, it's that painful. Many patients have said it's worse than childbirth, nonanesthetized root canals or body piercing with a flaming sword.
I've found this to be a very common condition. On the average I see about 8-15% of my patients having this in connection with their low back pain. Because of its major function it is a common muscle to become either overused or injured during extension and external rotation of the leg or flexion of the trunk.
Now that you've found it, what do you do? Unfortunately because of its location it is not treatable by most normal therapies. Many times even an adjustment will not relieve the condition, because once the adjustment is done the hypertonic muscle will return the joint to subluxation. I've found that in most cases I need to treat the surrounding regions of associated muscle pain, I do trigger point therapy within the femoral triangle to the insertion region of the muscle. This is extremely painful to the patient, but phenomenal in its positive effect. If you are not into causing pain, even for good therapy, send the patient to another doctor or massage therapist who will do this therapy.
Advise the patient that they will feel severe pain, but that it will only last for about 15 to 30 seconds. The patient is to tell you when you hit a spot which feels like a hot knife being stabbed into their muscle. The actual trigger point therapy is performed by applying strong pressure into the femoral triangle. When you find the right spot the patient will react strongly to the pain. Continue to apply the pressure without moving your fingers. Have the patient tell you when the pain begins to become less sharp or begins to subside, not when it's all gone, but only when it begins to subside. Move your finger a fraction of an inch in any direction and look for more trigger points. Generally you will find from 3-6 trigger points within the femoral triangle. Once you have treated each point, go over them one more time to retreat stubborn ones which have come back. This process will take about 2-3 minutes per leg. When the therapy is done apply a stretch to the muscle by pressing down on the bent knee and the contralateral hip against strong patient contraction of the muscle for about 10 seconds. Have the patient relax the leg and apply a little more pressure to the leg to give a small additional stretch to the muscle in a relaxed state.
I have my patients return the next available day for a follow-up. I continue to treat until the trigger points are not there when I palpate for them. The general sensation of pain will subside before this point is reached, but therapy must continue so that the dormant trigger points won't return.
This condition, like many other we repeatedly face, may be overlooked if one isn't looking for it. Often it is the low back pain we notice instead. The next time you have a diffuse low back pain patient who isn't responding as expected, try looking for a different muscle -- the iliopsoas muscle -- the great pretender.
Kenneth Rich, DC
Fremont, California
See also:
»Newer topics:
»Older topics:
»
![]() Groin strain causes
Groin strain causes
What to do if you are an unlucky sufferer from groin strains, and what action you can take to avoid them
![]() Groin strain causes
Groin strain causes
What to do if you are an unlucky sufferer from groin strains, and what action you can take to avoid them
See also:
»Newer topics:
»Older topics:
»
![]() Groin injuries
Groin injuries
A groin injury will result in muscle pain in the inner thigh or groin and can last for a short or significant amount of time.
![]() Groin injuries
Groin injuries
A groin injury will result in muscle pain in the inner thigh or groin and can last for a short or significant amount of time.
See also:
»Newer topics:
»Older topics:
»
![]() Adductor - Groin Strain
Adductor - Groin Strain
Straining the pectineus, adductor brevis, adductor longus the gracilis and adductor magnus.
![]() Adductor - Groin Strain
Adductor - Groin Strain
Straining the pectineus, adductor brevis, adductor longus the gracilis and adductor magnus.

